When internet fails, the clinic cannot stop
A clear guide for clinicians, NGOs, and governments that need to keep care, records, and reporting moving when connectivity fails.
Editorial & Product Team
When internet fails, the clinic cannot stop. The line keeps moving, the pharmacy still needs to know what is in stock, and the team still has to record what just happened. In that moment, a digital system that stops working does not help. It becomes one more interruption.
For clinicians, NGOs, and governments working outside ideal infrastructure, the question is not whether digital health sounds modern. The question is whether it lets teams keep caring, recording, and reporting when connectivity is unreliable.
PAHO and the IDB have pointed to health information systems and digital health as part of strengthening health services in Latin America and the Caribbean. That makes technology a continuity decision, not just a software purchase.
What teams experience when connectivity fails
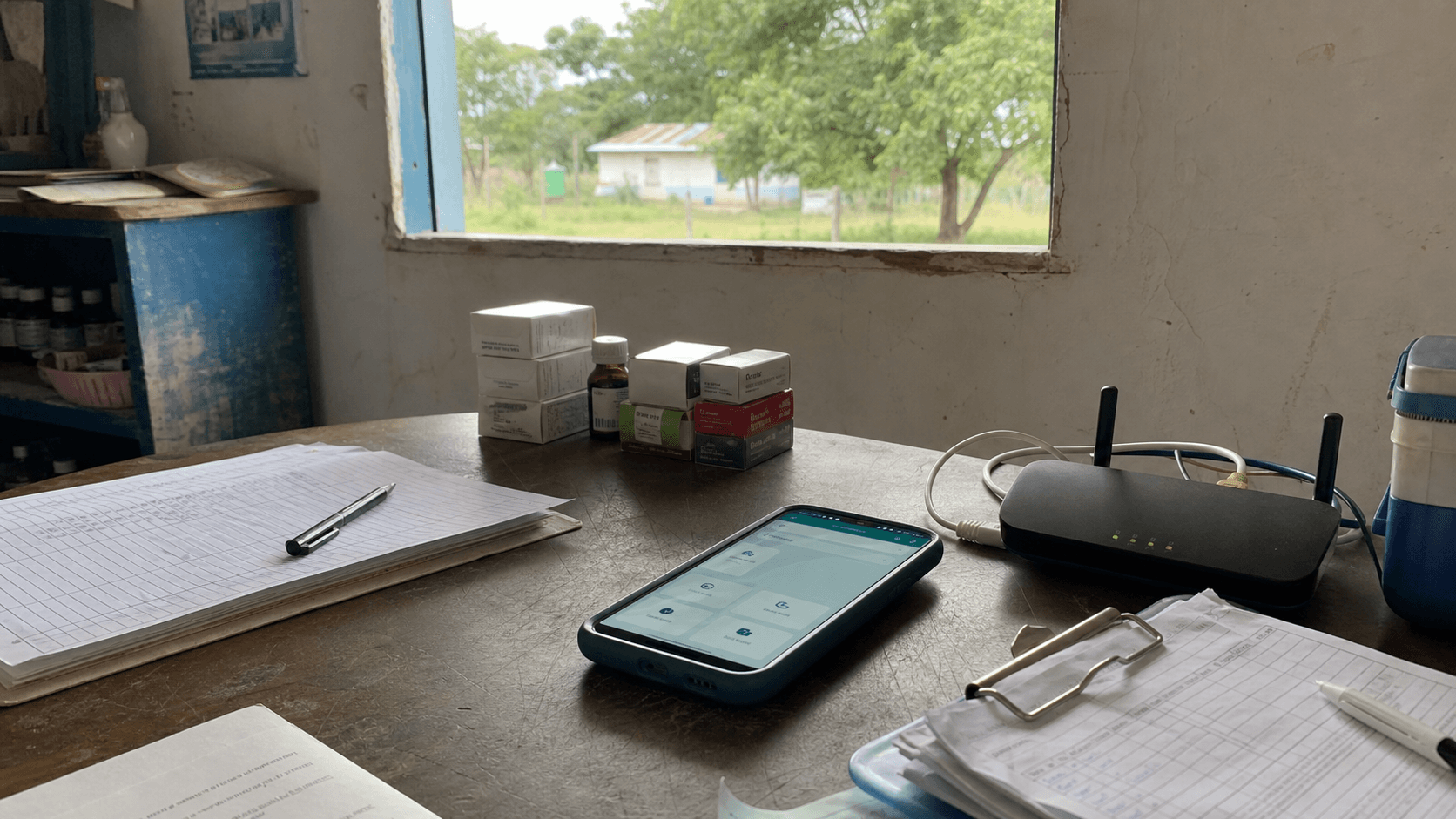
In a clinic with intermittent connectivity, the problem shows up in very concrete tasks: a visit that must be recorded, a medicine delivery that has to be logged, a report that needs to reach a central office, or a supervision process that depends on recent data.
If everything moves back to paper until someone can “enter it later,” the system starts losing visibility. Not because staff are not working, but because information arrives late, incomplete, or duplicated.
Offline-first, in plain language
Offline-first means something simple: the clinic can keep working even when there is no connection. Data is stored locally, waits safely, and syncs when the network returns.
The cloud still matters, but it stops being the required doorway for every task. The health center no longer depends on perfect connectivity to record what matters.
What this kind of system should allow
1. Record without blocking care
Staff should be able to record visits, inventory, administrative triage, and important events even when the signal is weak or absent. If the system freezes because internet is missing, the design is not respecting field reality.
2. Show what is still pending
Saving information is not enough. Teams need to know what has already synced, what is still waiting for connection, and what needs review. That clarity prevents the false comfort of assuming that “everything already went through.”
- Synced: the information has reached the central level.
- Pending: the information is safe locally and waiting for connection.
- Needs review: there is a conflict or error that an authorized person should resolve.
3. Support, without replacing clinical judgment
AI can help with tasks such as organizing a note, supporting dictation, or suggesting an administrative classification. It should not be presented as a substitute for medical judgment or as a guarantee of better clinical outcomes without evidence.
Important limit
This article is about operational continuity and digital architecture. It does not provide medical advice or claim that KYNODE reduces mortality, improves diagnosis, or produces clinical outcomes by itself.
Why this matters for NGOs and governments
For an NGO, an intervention is not sustained by activity photos alone. It needs reliable data to show continuity, coverage, and follow-up.
For a government or public network, delayed data affects supervision, supply planning, accountability, and resource decisions. An offline-first solution does not solve everything, but it reduces a common blind spot: depending on constant connectivity to know what is happening.
Security and trust from the beginning
The ITU identifies connectivity, security, interoperability, affordability, institutional capacity, and digital skills as key barriers for digital health adoption. That is why security cannot be added at the end; it has to be part of the design from day one.
- Role-based access: each person sees only what they need for their work.
- Auditability: changes remain traceable, including those made while offline.
- Minimum necessary data: the workflow captures what is truly needed, not endless forms nobody can sustain.
What KYNODE can promise with discipline
KYNODE can promise a clear direction: helping teams record, continue operating, and synchronize information in settings where connectivity is not always available.
What it should not promise without evidence is to “save lives,” return exact percentages of staff time, or improve clinical outcomes by itself. Trust grows when technology speaks precisely and respects the complexity of health systems.
Checklist for evaluating an offline-first solution
- Can the clinic record critical data without connection?
- Can staff clearly see what is synced and what is still pending?
- Does the system explain errors in operational language, not technical jargon?
- Does it include access controls, audit trails, and a plan for lost devices?
- Does it avoid promising clinical outcomes without evidence?
- Does it serve the clinician, the supervisor, the funder, and the public-health team?
Sources used
- PAHO/IDB: digital health, information systems, and health service strengthening in Latin America and the Caribbean
- ITU: digital health opportunities and risks, including connectivity, security, interoperability, and institutional capacity
- PAHO/WHO: primary health care, universal health, and access barriers in the Americas

